Alternative names for polycystic ovary syndrome
Stein-Leventhal syndrome; PCOS; polycystic ovarian syndrome. There are discussions ongoing as to whether to rename the condition to highlight the associated metabolic dysfunction.
{kind=link}
What is polycystic ovary syndrome (PCOS)?
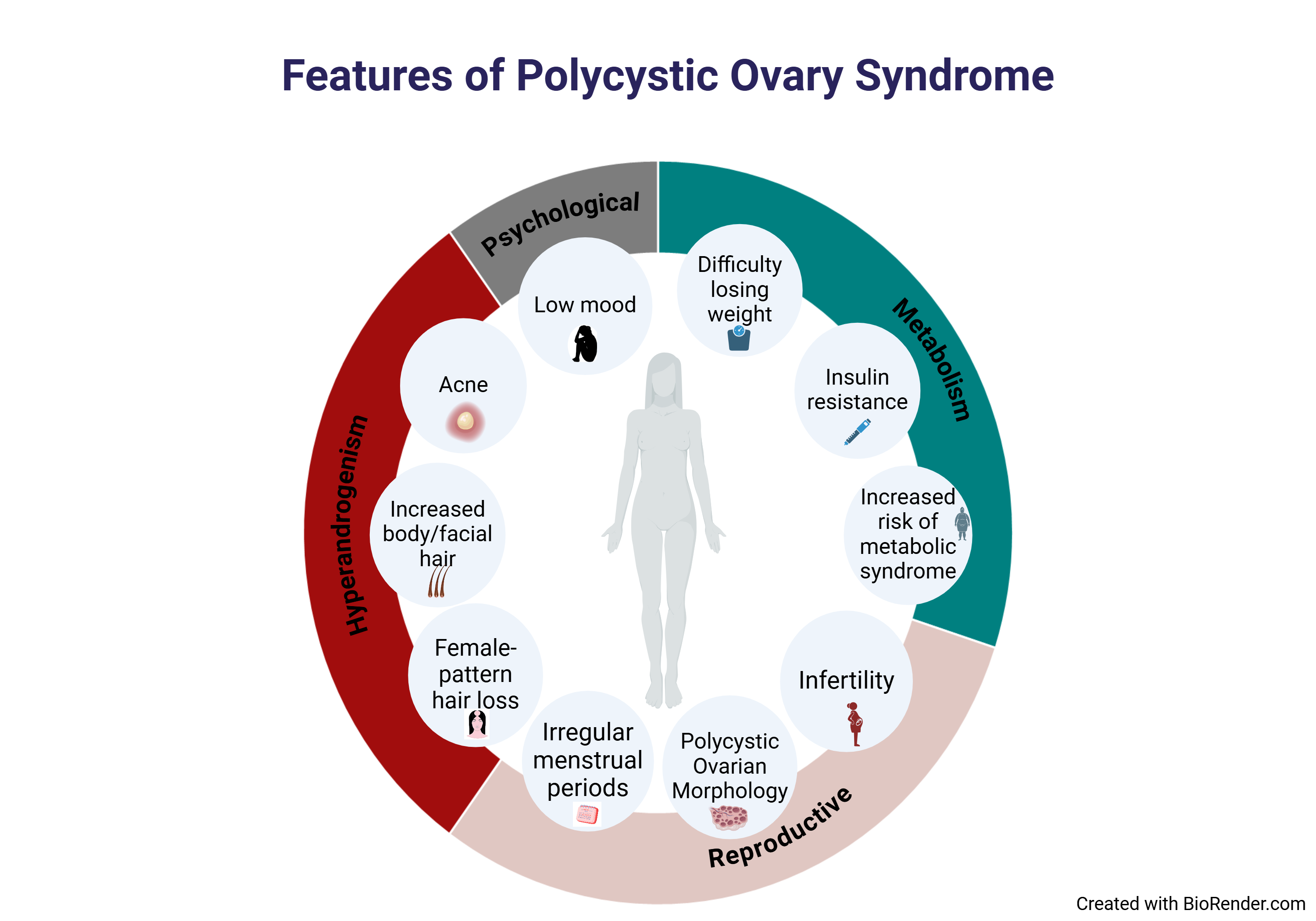
Polycystic ovary syndrome (PCOS) is a condition that can affect hormones in the body and has three key features, namely: 1. Hyperandrogenism, 2. Irregular periods and 3. Polycystic ovarian morphology on ultrasound. At least two of these three key features are needed for a diagnosis of PCOS.
- Hyperandrogenism refers to high androgen levels in the blood. Androgens are hormones such as testosterone, which if too high can cause symptoms such as excess hair growth (called hirsutism) and acne. It is normal for women to have androgens, although they are normally present at much lower levels than those found in men (usually less than one tenth of those found in men). In PCOS, the levels of androgens can be slightly increased, which can cause symptoms such as hirsutism and acne, and can also lead to menstrual cycles being disrupted. High androgens can also result in metabolic disturbance, such as causing insulin to no longer work properly. This is called ‘insulin resistance’ and can lead to an increase in insulin levels to compensate. Notably, this can establish a vicious circle where high insulin levels and high luteinising hormone (LH) levels in turn stimulate the ovaries to make even more androgens.
- Irregular periods - Periods usually occur once every month in a healthy woman, but in PCOS, periods can be less frequent, which is called ‘oligomenorrhoea’.
- Polycystic Ovarian Morphology - The ovaries can have a particular appearance on an ultrasound scan called ‘Polycystic Ovarian Morphology’. However, this can be normal, and not all women with this appearance have PCOS unless they have at least one of the other key features.
{kind=link}
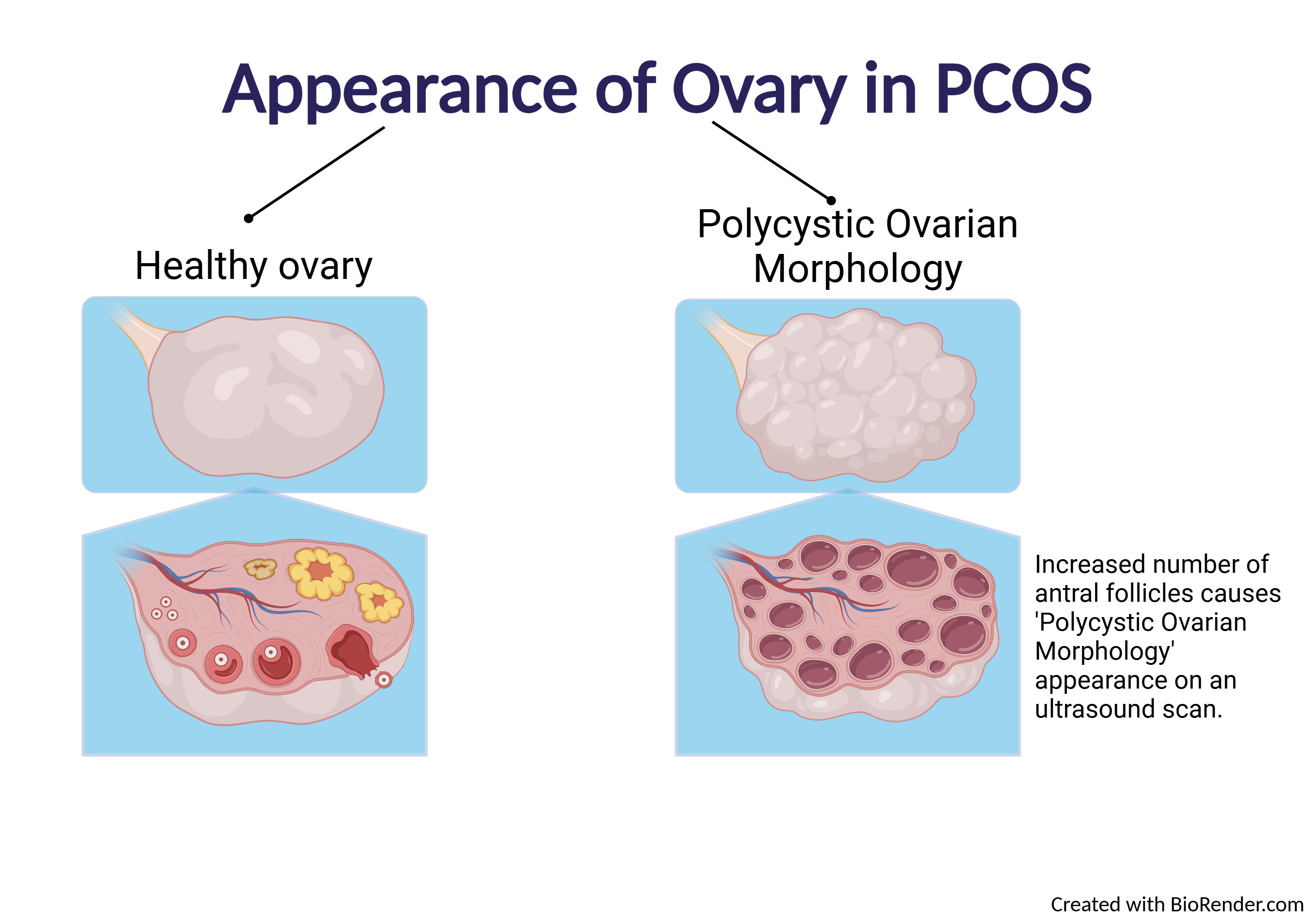
Figure 2. Representation of the appearance of Polycystic Ovarian Morphology on an ultrasound scan.
What causes polycystic ovary syndrome?
PCOS is due to several factors, but our genes are known to be important, and PCOS often runs in families. In fact, many women are diagnosed with PCOS in early adulthood. PCOS is due to abnormalities in many genes, which all make a small contribution to the risk of developing PCOS.
Many women with PCOS have higher bodyweight, which can cause and exacerbate insulin resistance and further increase androgen levels. Insulin resistance can also increase the risk of having type 2 diabetes mellitus or diabetes during pregnancy (called gestational diabetes). Therefore, PCOS is also recognised to be a ‘metabolic condition’ in that it can result in abnormal glucose (sugar) and lipid levels. In the longer term (after many years), it can result in a small increase in the risk of cardiovascular disease (e.g. heart attacks), which may need further treatments to prevent. A healthy lifestyle, weight loss and certain medications e.g. metformin can help improve symptoms of PCOS and reduce these small long-term risks.
{kind=link}
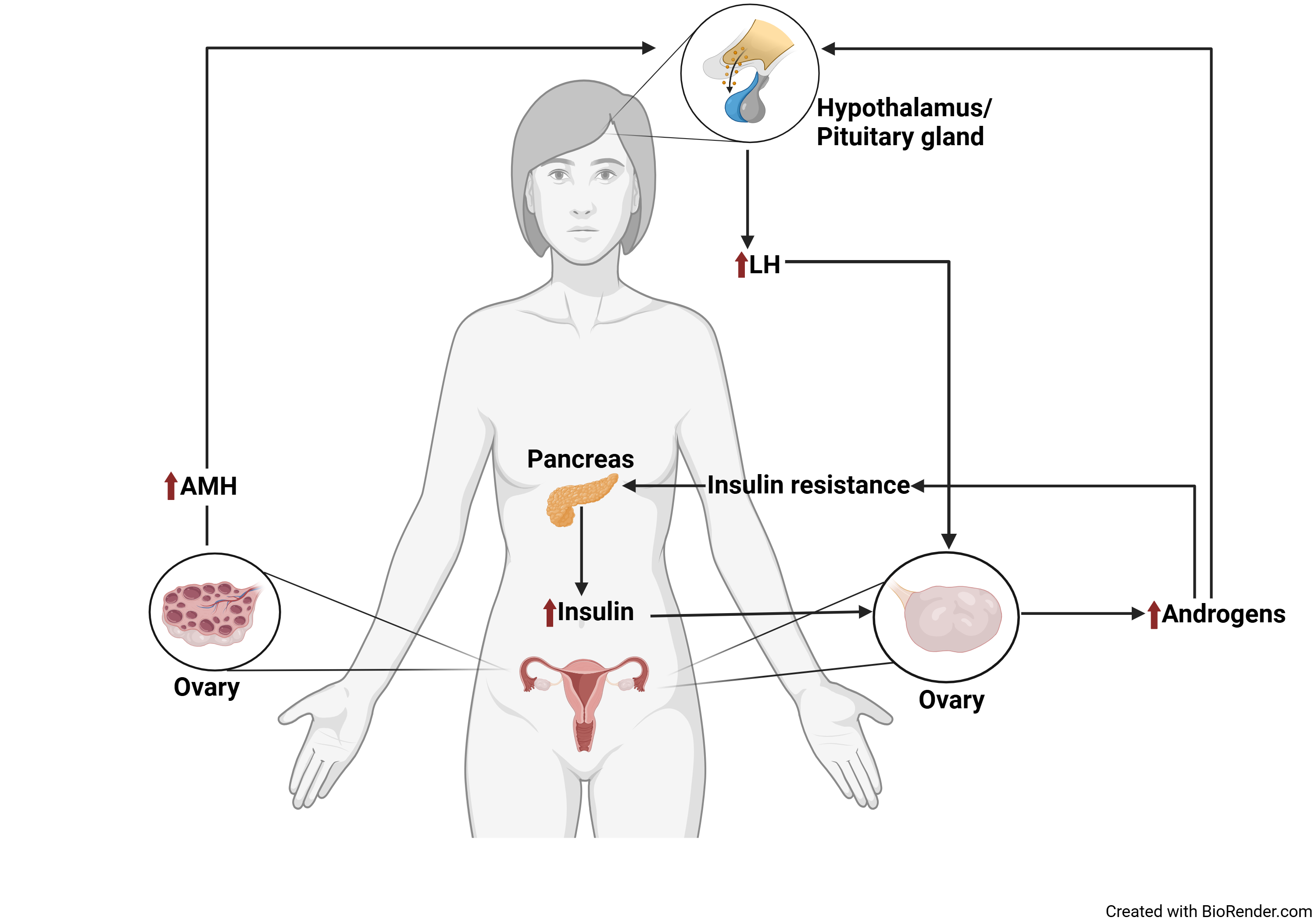
Figure 3. Diagram showing the mechanism of PCOS. Abbreviations: LH, luteinising hormone; AMH, anti-Mϋllerian hormone.
How common is polycystic ovary syndrome?
Polycystic ovary syndrome typically affects 10-13% of women but can be more common (up to 20%) depending on the specific population studied (World Health Organisation, 2025). PCOS is more common in people from minority ethnic backgrounds and disadvantaged socioeconomic groups. The threshold levels for diagnosis of PCOS can also vary by ethnic group. For example, the degree of hirsutism that would be regarded as abnormal can differ depending on the ethnic background.
What are the signs and symptoms of polycystic ovary syndrome?
Every woman with PCOS is different and can have a unique set of signs and symptoms:
- Irregular (or less commonly absent) periods called ‘oligomenorrhoea’ (or ‘amenorrhoea’).
- Abnormal increase in body or facial hair (called hirsutism).
- Loss of hair on the scalp (called alopecia).
- Acne.
- Higher bodyweight.
- Infertility – difficulty getting pregnant.
- Low mood and self-esteem.
- Reduced quality of life.
- Increased risk of developing diabetes.
How is polycystic ovary syndrome diagnosed?
Polycystic ovary syndrome can present at any age from puberty up to menopause (reproductive years). It can also potentially be diagnosed after menopause based on history, but it is harder to measure hormone tests to confirm the diagnosis at older ages. It is important to rule out other diagnoses that can mimic the features of PCOS, and so it can take time to receive an accurate diagnosis of PCOS. Early diagnosis and management lead to better outcomes.
To diagnose PCOS, two of the following three key features are needed for a diagnosis of PCOS:
1. Hyperandrogenism
Hyperandrogenism means having high androgens. This can be identified via clinical features such as hirsutism or acne, or via a blood test demonstrating high levels of androgens e.g. testosterone. High androgens in PCOS are caused by high luteinising hormone (LH) levels and high insulin levels, which stimulate the ovaries to make excess androgens.
Luteinising hormone (LH) levels are typically increased in PCOS, as the function of the hypothalamus is increased. The overactive hypothalamus leads to an increase in the frequency of Gonadotropin-Releasing Hormone (GnRH) secretion, which in turn stimulates the pituitary gland to increase LH levels. LH stimulates the ovaries to make excess androgens.
Additionally, PCOS can be associated with higher bodyweight, which can cause insulin to not work properly, called ‘insulin resistance’. This can lead to increased insulin levels to try to compensate for it not working properly. The higher levels of insulin can also stimulate the ovary to make excess androgens, in combination with raised LH levels.
2. Irregular periods
Irregular or absent periods (oligo-menorrhoea or a-menorrhoea) usually means that ovulation is not occurring regularly as in health. This lack of ovulation is a common cause of infertility.
3. ‘Polycystic Ovarian Morphology’
A key feature of PCOS, is the appearance of the ovaries on an ultrasound scan called ‘Polycystic Ovarian Morphology’. The ovaries can appear like they contain many small ‘cysts’. Cysts are small fluid-filled sacs; however, this is NOT an accurate description of the appearance of the ovaries in PCOS and should not be confused with ‘ovarian cysts’ which can rarely indicate a cancer of the ovary.
In fact, these small circles are small (called antral) follicles (small fluid-filled sacs that contain an egg) that have not fully developed to release an egg during ovulation. In PCOS, the number of antral follicles is increased. Having more than 20 antral follicles in one ovary denotes ‘Polycystic Ovarian Morphology’.
More recently, a blood test called anti-Mϋllerian hormone (AMH) has been used as an alternative to having an ultrasound scan for identifying ‘Polycystic Ovarian Morphology’. AMH is a hormone made by these antral follicles in the ovaries and is increased if there are an increased number of follicles in the ovary. Therefore, a high AMH level can now also be used as a feature for the diagnosis of PCOS.
As only two of the three key features of PCOS are required for the diagnosis, none of the three features are mandatory and have to be present in all women with a diagnosis of PCOS. This means that many women with PCOS can have a different combination of signs and symptoms, and hence different treatment needs.
Some of the features can be present in other conditions, and even in health (a fifth of healthy women have polycystic ovarian morphology). Therefore, other hormonal conditions that could give similar signs and symptoms need to be ruled out before reaching a diagnosis of PCOS.
How is polycystic ovary syndrome treated?
Polycystic ovary syndrome and general health
Although there is no cure for PCOS, there are a lot of ways to manage the symptoms. The specific treatment depends on what is important for each woman at that time in their life. Management options should be discussed and agreed between the woman with PCOS and the healthcare professional caring for her (called shared decision making).
The goals of treatment are to reduce symptoms, improve quality of life, and prevent long-term complications.
A healthy lifestyle is very important in PCOS. Eating healthily, being active, maintaining a healthy weight and avoiding harmful habits (e.g. smoking and drinking alcohol in excess) are important for the management of PCOS.
There is no specific diet that has shown to be superior to others in the management of PCOS. Any healthy diet that suits a particular individual such that they are able to stick to it in the longer term to help with weight loss is beneficial for PCOS.
Setting goals, with or without support from healthcare professionals, can help maintain a healthy lifestyle.
Metformin is a drug commonly used in PCOS to help treat insulin resistance, and can help periods becoming more regular and improve androgen levels.
It is important that women with PCOS reach out to healthcare professionals early on to support them in their journey and guide them through management options.
Polycystic ovary syndrome and periods
If women are not planning on becoming pregnant in the near future, the oral contraceptive pill can be used to regulate periods and reduce the level of androgens in the blood. This helps reduce symptoms of hirsutism and acne. Other drugs that can be used to reduce the effects of androgens include spironolactone and cyproterone acetate.
It is important to have a period at least once every three months to ensure that the lining of the womb is changed regularly, so that it remains healthy. If not, there is a small increased risk of developing abnormal cells and eventually even endometrial cancer. Having a regular bleed after the oral contraceptive pill or with a course of progesterone tablets can avoid this complication.
Another option is to use a device such as a coil which sits in the womb and releases progesterone continuously to stop the lining getting thick. This can be used for years and works to protect the lining of the womb and can also provide contraception.
Polycystic ovary syndrome and fertility
Polycystic ovary syndrome can cause difficulties in getting pregnant (called infertility). This is because in PCOS, ovulation can stop completely or can happen infrequently causing irregular or absent periods. This means that it is harder for women to become pregnant, but not impossible, such that contraception is still important if pregnancy is not desired.
Living a healthy lifestyle and losing even just 5% of bodyweight can improve ovulation rates and the chance of getting pregnant. However, most couples will benefit from a referral to a fertility specialist to check for other factors too.
There are several treatments for fertility available that can restore normal ovulation. These include pills taken by mouth like letrozole, clomiphene citrate, or injections that contain follicle stimulating hormone (FSH). More intensive options include assisted reproductive technology (ART) such as in vitro fertilisation (IVF) treatment. Women with PCOS tend to have high antral follicle counts, and can respond strongly to stimulation of the ovaries during IVF treatment. This can increase the chance of a condition called ‘ovarian hyperstimulation syndrome’ (OHSS) and may require specific steps taken to avoid this.
Are there any side-effects to the treatment?
Metformin can sometimes cause nausea, vomiting and stomach upset. These are reduced when starting on a lower dose, taking the tablet with meals, and increasing the dose slowly. A slow-release form of metformin, when taken at night, has fewer side effects.
Spironolactone can also cause stomach upset and result in more frequent periods, and is not safe during pregnancy. Therefore, it is often used together with the oral contraceptive pill.
Cyproterone acetate blocks the effects of androgens, and can sometimes cause problems with periods if taken for a long duration. It can cause issues with the liver, which are monitored for by blood tests.
The oral contraceptive pill can sometimes cause mood changes, headaches, changes in weight and breast tenderness but these depend on the specific pill used.
What are the longer-term implications of polycystic ovary syndrome?
Women with PCOS tend to have a higher prevalence of developing ‘metabolic syndrome’. This includes a combination of conditions which increase the risk of developing chronic diseases like:
- Diabetes and insulin resistance
- High blood pressure
- High cholesterol
- Fatty liver
- High bodyweight
- Heart disease
During pregnancy, there is also a greater chance of developing diabetes (gestational diabetes). There is also a higher chance of high blood pressure in pregnancy, which can affect the baby’s health.
If no period is achieved for a few months or more, this increases the risk of endometrial cancer. This is why it is important to have a period at least every three months.
Any person who has concerns about the implications of PCOS is advised to contact a healthcare professional to provide guidance and support.
Are there patient support groups for people with polycystic ovary syndrome?
There are several support groups available for women with PCOS. Verity PCOS-UK is a patient support group that may be able to provide advice and support to patients and families dealing with polycystic ovary syndrome.